Retake
P3) Intermittent abdominal pain
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a pediatric patient with abdominal pain.
- Review the DDx considerations in a pediatric patient with abdominal pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a pediatric patient with abdominal pain.
History
A 2-year-old male is brought to the emergency department by his mother, who reports that he has been experiencing intermittent, severe abdominal pain for the past 24 hours. The pain initially started as mild discomfort but progressively increased in frequency and intensity. Additionally, the child has had three episodes of vomiting. He had viral gastroenteritis two weeks ago that has since resolved.
Physical Exam
BP: 98/62 mmHg, HR: 115 bpm, RR: 25 breaths/min, Temp: 98.6°F (37°C), O2 saturation: 99%. A palpable, tender, sausage-shaped mass is noted in the epigastric region.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
Intussusception is the most likely diagnosis in this patient, given the progressive, intermittent abdominal pain, vomiting, and the presence of a palpable abdominal mass. Pyloric stenosis typically presents between 2 to 8 weeks of age and is characterized by painless, "hungry vomiting." A Wilms tumor is less likely to present with vomiting and intermittent abdominal pain.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
An abdominal ultrasound is the preferred initial imaging modality for children, as it avoids radiation exposure and has excellent sensitivity for diagnosing intussusception. It can also help differentiate intussusception from other intraabdominal masses.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Abdominal ultrasound
What best describes the imaging findings on the abdominal ultrasound?
The target or doughnut sign, which is visible. It represents intussusception, where a segment of the bowel telescopes into an adjacent segment. It appears as different layers of the intestine folding into each other. The hyperechoic concentric bands are secondary to mucosa and the muscularis propria. The hypoechoic bands are secondary to the submucosa.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
A lower gastrointestinal (GI) fluoroscopy, can be utilized to attempt the reduction of intussusception in children. This procedure is considered appropriate when there are no indications of bowel perforation, such as peritonitis, the symptoms have not been prolonged, and there is an absence of rectal bleeding, which could suggest ischemic bowel.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
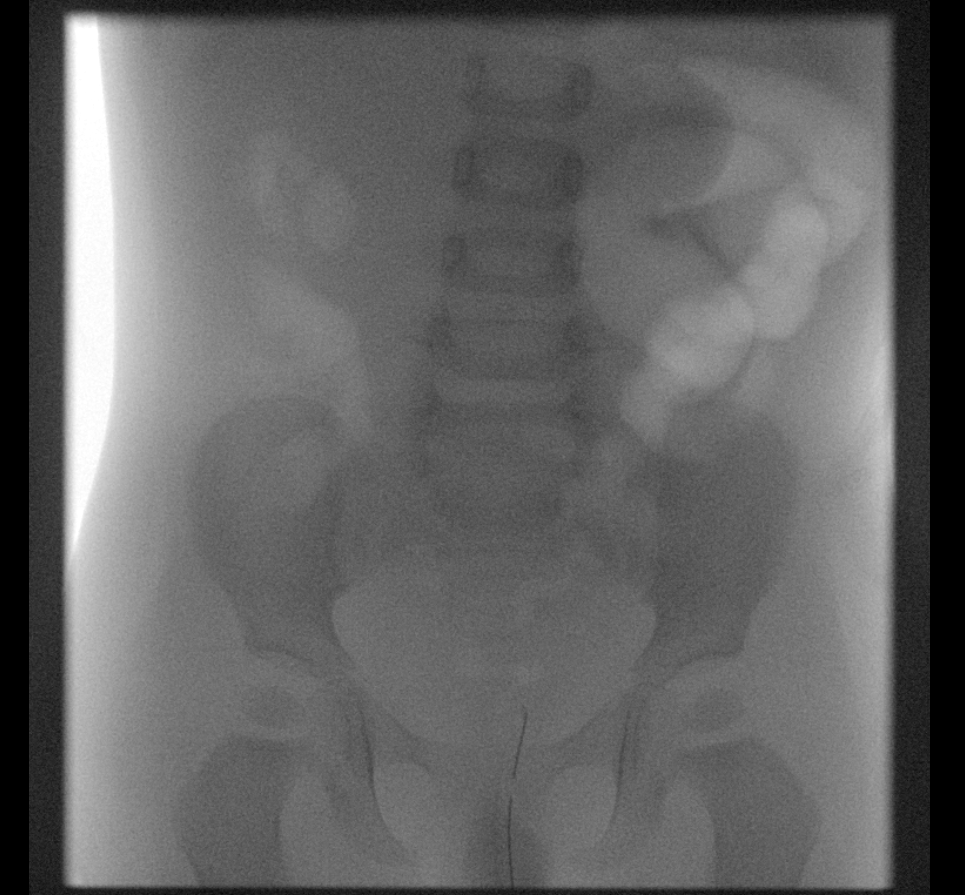
Lower GI Fluoroscopy
Is there evidence of intussusception?
Intussusception is evident, with an intussusceptum, or a loop of bowel telescoping into another, located in the epigastric region.
Was the intussusception reduced?
The intussusceptum was successfully reduced beyond the terminal ileum. The colon was filled throughout its entire length, and air refluxed into the small bowel, confirming a successful reduction.
View the full study if you'd like to like a look yourself
Third Imaging Study
What is the next imaging study you will order?
No further imaging is required. The intussusception was diagnosed and reduced with a lower GI air enema under fluoroscopy.
What is your Diagnosis now that you have seen the imaging results?
Intussusception in children is primarily believed to be associated with hypertrophic lymphoid tissue following an infection, which, in this patient's case, occurred two weeks ago.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
N/A. Intussusception was reduced.
Assessment and Plan
Please provide your assessment and plan for this patient
This is a 2-year-old male presenting with intussusception, likely secondary to hypertrophic lymphoid tissue from a previous infection. A diagnostic and therapeutic air enema was performed, successfully reducing the intussusception.
Lessons Learned:
- Intussusception is one of the most common causes of intestinal obstruction in infants, with ileocolic intussusception being the most prevalent type.
- Patients with intussusception typically present with abdominal pain, vomiting, and a palpable abdominal mass. The “classic triad” of symptoms, including abdominal pain, a palpable mass, and currant jelly stools, occurs in only about 15% of cases. Hematochezia is a late finding, indicating bowel necrosis.
- Ultrasonography is the preferred diagnostic method, as it avoids radiation exposure. It may reveal the target or doughnut sign, which represents alternating hyperechoic and hypoechoic bands due to a segment of bowel telescoping into an adjacent segment.
- For symptomatic, stable patients without suspected bowel perforation or ischemia, nonoperative reduction guided by fluoroscopy or ultrasound with pneumatic or hydrostatic enemas is recommended.
Socioeconomic Factors: The introduction of the rotavirus vaccine has been associated with a reduction in intussusception cases in some countries.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}